

Last time, I briefly touched on something that had always puzzled me during facelift surgery.
Despite how heavily many facelift clinics emphasize the SMAS fascia, there were patients in whom this structure was clearly identifiable during surgery, and others in whom it was surprisingly difficult — or almost impossible — to find. That inconsistency was what initially made me question whether the “SMAS” we talk about is truly a distinct anatomical structure in every patient.
If the plastic surgery textbooks, and many of the world’s leading facelift surgeons, all describe the SMAS facelift as the gold standard —almost as if that single technique can solve everything — then why does this inconsistency happen?
So when I discussed this with colleagues and other surgeons around me, the answers I kept hearing generally fell into two categories.
“1: I experience the same thing too. But that’s simply the limitation of the surgery itself.”
“2: No, that happens because you’re not dissecting properly. That’s your limitation as a surgeon.”
Choosing the first answer may have been comforting, but comfort rarely leads to growth.
So I decided to believe the second answer instead. I modified my surgical techniques, changed the way I approached dissections, and spent even more time studying the literature and anatomy papers. And somewhere during that process, this paper was published.
This paper resolved many of the questions and frustrations I had been struggling with for years. In some ways, it challenges the long-standing and deeply accepted paradigm of the “SMAS” itself. And because of that, I thought it would be worthwhile to introduce it here for anyone interested in facelift surgery, as I believe understanding these newer anatomical perspectives is becoming increasingly important.
To summarize the paper in one sentence, it essentially argues that:
“There is no SMAS.”
Or perhaps more accurately:
“The SMAS may exist — but it is not the distinct, uniform anatomical layer you were taught to expect.”
What do you think defines a luxury brand? Of course, we associate it with elegance and exclusivity, but at its core, a luxury brand simply means “a name that has become widely recognized.”
In fashion, designers behind brands like Hermès or Chanel become luxury brands because their names themselves carry reputation and trust. And in the world of facelift surgery, the “luxury brands” are probably the surgeons whose names have become well known —the designers and operators whose facelift techniques are recognized around the world.
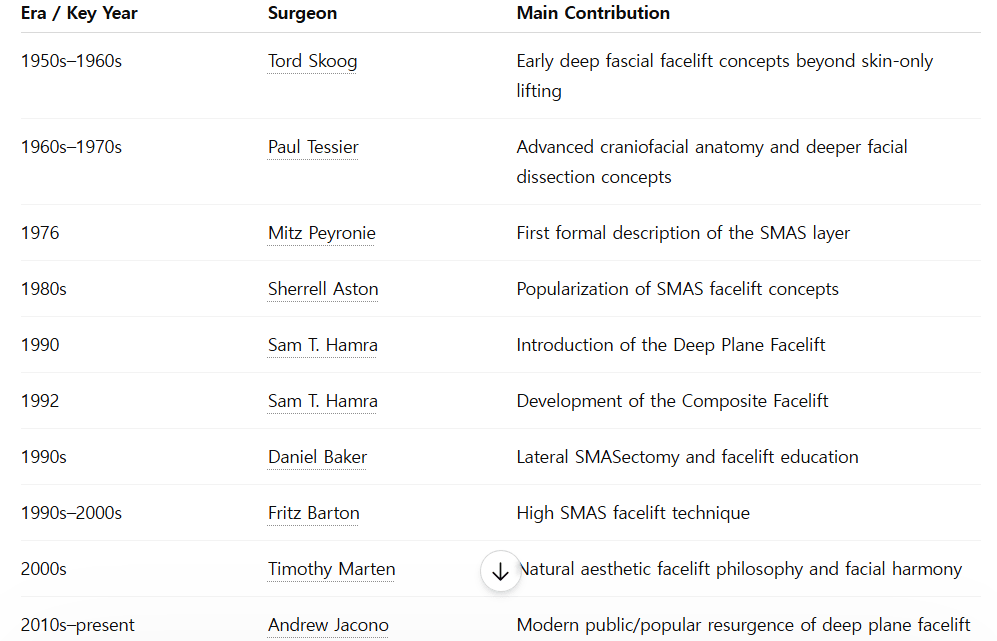
Facelift surgery is believed to have first appeared around the early 1900s, while modern surgery under anesthesia only truly became standardized and rapidly developed after the mid-20th century. So if we were to look at the most influential “luxury designers” of the facelift world after the 1950s —the surgeons whose names shaped modern facelift surgery itself — let’s try asking ChatGPT for ten of the most famous names in facelift history.

From the perspective of a plastic surgeon who studies facelift surgery, every one of these names is impossible to leave out.
To me, looking at these surgeons feels almost like a fashion designer looking at brands such as Hermès, Chanel, Louis Vuitton, or Prada.
And interestingly, one of those names appears as an author in the paper I mentioned earlier.
Among the ten “luxury designers” of facelift surgery history, this paper comes from the Australian school led by Bryan Mendelson —a group widely respected for performing some of the most detailed and active anatomical research in facelift surgery.
More specifically, the paper was written by a younger surgeon named Lennert Minelli. The full paper is long and highly detailed, and even if I summarized everything carefully, it would probably become exhausting to read. So instead, let me pull out just a few of the key sentences. I got chills while reading this paper.
In the series of standardized sharp-layered dissections on the contralateral side of the same cadavers, an aponeurotic layer 3 in the anterior midcheek could not be demonstrated.
One, two, or three sheets of fascia-like tissue (or “SMAS” layers) could be surgically created, depending on the thickness of the dissection decided by the dissector.
These different sheet-like connective tissue layers were created out of one composite tissue layer, similar to slicing cheese.
They were not distinct sheets before their dissection.
When strictly dissecting only the aponeurotic layers present, a clear gap was consistently visualized between the STF superiorly and the platysma inferiorly.
It was relevant to my previous post.
What surprised me even more was that I hadn’t written my earlier posts with this paper open beside me. And yet, I found myself using almost the exact same expressions and analogies. That was fascinating even to me.
And you know how Western countries consume a lot of cheese? When you slice cheese, there usually isn’t a precise anatomical boundary telling you exactly where one layer ends and another begins. You simply choose a thickness that feels appropriate for eating, and slice through it accordingly.
I had actually used a very similar analogy myself before —saying that dissecting this layer sometimes feels more like trimming fat from pork belly than separating a clean, distinct fascial plane.
Of course, his analogy was cheese, while mine was pork belly. But I suppose we arrived at the same realization in the end.
This paper became the theoretical foundation that finally allowed me to let go of my obsessive fixation on the idea of the “SMAS” as a perfectly distinct fascial layer.
And more importantly, it pushed me to think beyond the question of
“What exactly is the SMAS?”
and toward a far more important one:
“Then how should we actually perform facelift surgery?”
In many ways, this paper became the starting point that helped me develop my own thoughts and answers to that question.
That’s all for today’s post.
I’ll continue in the next one.